The following article was published in The Globe and Mail on February 25th 2020.
In an African nation where abortion was only recently legalized, the barriers to access are public education, medical training and money. An $18-million Canadian project is trying to help, and Mozambicans say it’s saving lives
GEOFFREY YORK
AFRICA BUREAU CHIEF
MANICA, MOZAMBIQUE

For years, the blood supply at Manica District Hospital was falling to worryingly low levels. So many women needed emergency transfusions, after undergoing dangerous abortions at home, that its blood stocks often became depleted.
“They would come here almost in shock from hemorrhaging,” said Flora Diomba, clinical director of the hospital in central Mozambique. “Women were trying to get rid of their pregnancy at any cost.”
Today, she sees a drastic improvement: The blood inventory is at a comfortably high level. Transfusions are rarely needed, because a Canadian-funded program has trained four of the hospital’s doctors to provide safe medical abortions.
Cases of abortion complications have declined steeply, and the lives of many women have been saved, Dr. Diomba says.
“The training should have been introduced a long time ago,” she told The Globe and Mail.
Canada must boost foreign aid for feminist agenda to have sustained impact, experts say
The $18-million Mozambique project is financed under the Trudeau government’s “feminist international assistance” policy, which provides $550-million annually for sexual- and reproductive-health and rights, including family planning and abortion, with plans to increase funding over the next three years.
The safe abortion training could be the most controversial element of the project – especially in an era when President Donald Trump’s administration has banned U.S.-funded organizations from providing any information about abortion, causing severe budget shortfalls for clinics where U.S. donors were forced to withdraw.
Many clinics in Mozambique and elsewhere in Africa have been forced to cut back their family-planning services since 2017 because of the Trump policy, commonly known as the Global Gag Rule. In countries such as Malawi, proposals to liberalize anti-abortion laws have reportedly been delayed or halted by a fear of losing funds from the Trump administration.
The results are beginning to emerge – and there is growing evidence, in places such as Manica, that the policy is preventing deaths.
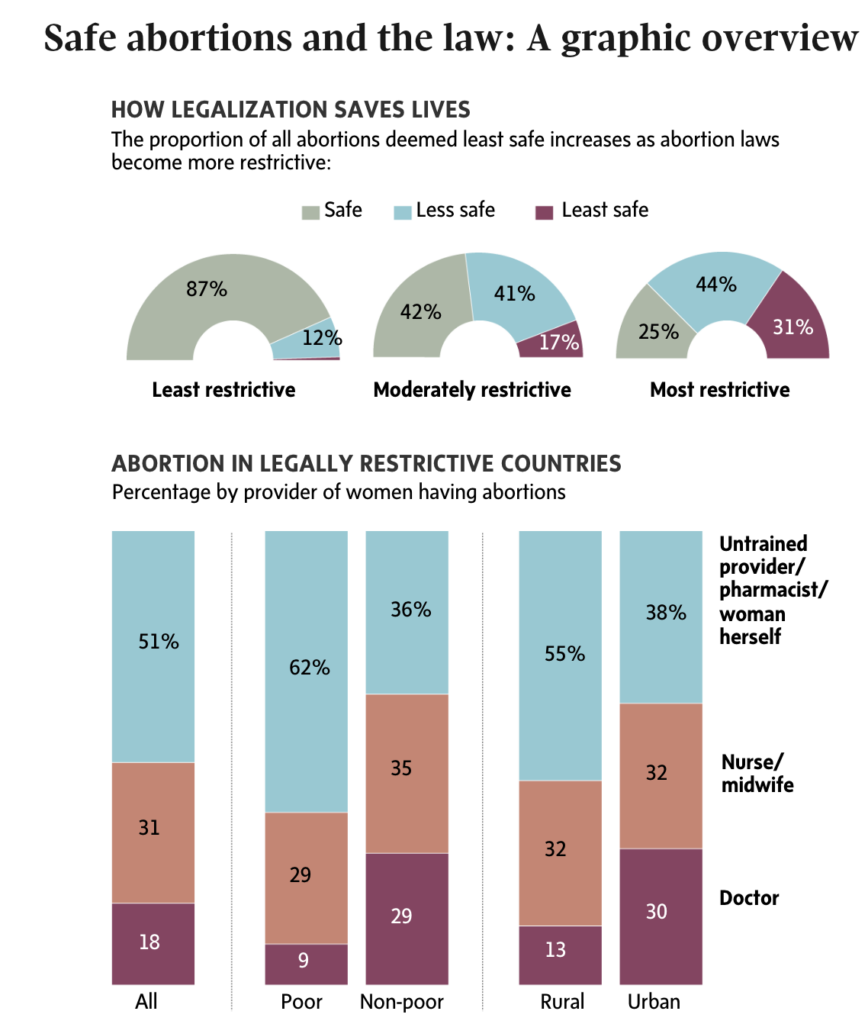
Abortion is illegal in much of the developing world, forcing women to use dangerous clandestine methods if they want to end their pregnancies. Studies estimate there are about 25 million unsafe abortions around the world annually, causing about 30,000 deaths among women every year – almost entirely in low- and middle-income countries.
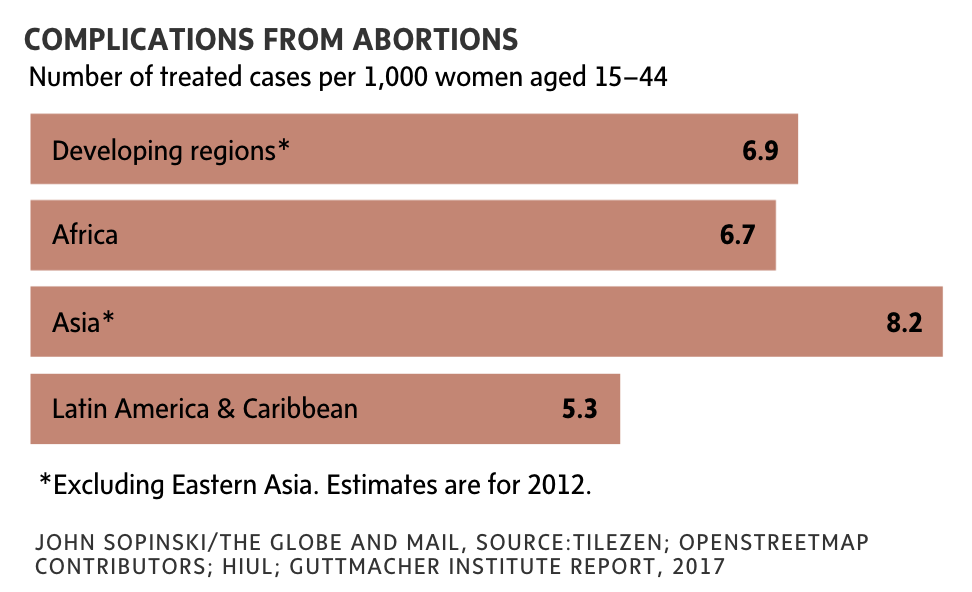
In Africa, about three-quarters of abortions are unsafe, and about 1.7 million African women are hospitalized annually because of unsafe abortions, according to the World Health Organization. In Mozambique, as in most other African countries, complications from unsafe abortions are among the leading causes of maternal mortality, accounting for an estimated 11 per cent of all deaths among pregnant women and girls. There are an estimated 100,000 abortions in Mozambique annually – and almost all have traditionally been illegal and highly risky. An estimated 350 women die annually in the country because of unsafe abortions.
When the former Conservative government launched Canada’s $3.5-billion maternal and child-health program in 2010, abortion was explicitly excluded from the program, mainly because many Conservatives were ideologically uncomfortable with it. But the government of Prime Minister Justin Trudeau has now made abortion a significant element in Canada’s aid strategy in countries such as Mozambique, one of a small number of African countries where abortion has been legalized without restrictions in the first 12 weeks of pregnancy.
In Africa, the impact of traditional foreign aid can often be subtle and difficult to measure. Doctors and nurses in Mozambique, however, are describing the results of the Canadian feminist aid program as dramatic and swift. “We’re seeing a reduction in the number of people dying and the number of people injured,” said Murtala Mai, the chief of country and program strategy at Pathfinder International, a U.S.-based health organization that is implementing the Canadian-funded project in Manica and Tete, two of Mozambique’s 10 provinces.
“In this project, we are very sure that we will be able to reduce deaths from unsafe abortions by close to 70 to 80 per cent,” Dr. Mai told The Globe in an interview. “We have very ambitious targets and we’re on track to achieve those targets.” The Mozambique project is “a trailblazer” that could serve as a model for other countries in the developing world, he said.
“We’re saving lives,” said Salomao Tivane, a physician and clinical officer at Pathfinder who has trained 15 doctors to provide abortion services in Manica province since late 2018 as part of the Canadian project. “I feel a sense of satisfaction, because I’m helping to reduce the risk of dying.”

In addition to training doctors and providing abortion medicine, the Canadian project uses household visits and small-group discussions to help educate Mozambicans on family planning and contraception methods, sexual and reproductive rights, gender equality and the need to halt child marriage and gender-based violence. It has also trained hospital and clinic staff to file reports with the police when they see victims of rape or other violence. Its main focus is on girls and young women up to the age of 24, although it also includes education sessions for young men.
In Mozambique, abortion during the first 12 weeks of pregnancy (and up to 24 weeks in some circumstances) was legalized in 2014. But until the arrival of the Canadian-funded training program in late 2018, safe abortions were still not provided in almost all of Mozambique’s regions, because doctors and nurses hadn’t received proper training. Most were not even aware of the new law.
Natalia Paulo, head of the maternity ward at one of the biggest health clinics in Chimoio, the capital of Manica province, remembers women dying from unsafe abortions as recently as 2018. They would arrive with complications from perforated uteri or infections, and they would be rushed to a provincial hospital, where some would die.
But then she and other colleagues at the clinic were trained by the Canadian-financed project in December, 2018. Now, they provide an average of six or seven safe abortions a month.
The women are given a drug called mifepristone (also known as RU-486) at the clinic, followed by a second medicine called misoprostol later when they are home.
“I haven’t seen a complication from unsafe abortion in the whole year since then,” Ms. Paulo told The Globe. “In the past, it was routine to see women who did unsafe abortions,” she said. “They inserted sticks or roots into themselves. But now it’s rare. People are becoming more informed, and more women will be coming here now.”

Two authorizations from doctors and nurses are required for each procedure, usually done on the same day when the woman arrives. After every abortion, the clinic provides the women and girls with counselling on family planning and contraception, to help them avoid unwanted pregnancies in the future.
Canada’s Minister of International Development, Karina Gould, said she is “thrilled” to learn that health providers are reporting dramatic declines in unsafe abortions. In an interview, she told The Globe that she is seeing similar evidence from her department’s monitoring and evaluation system, suggesting that the Mozambique project is reducing the number of dangerous clandestine abortions.
“It’s still in the early stages, but we are seeing results,” Ms. Gould said. “Life-saving results.” As of January, she said, the project had provided 283 safe medical abortions, while organizing more than 20,000 household visits and 9,000 community meetings with women and adolescent girls to talk about family planning, child marriage and gender-based violence.
Hospital and clinic abortion services, such as the Canadian-funded project in Mozambique, do not increase the total number of abortions in a country, Ms. Gould said. Instead, they simply reduce the number of dangerous abortions, replacing them with safe abortions. “If women want to terminate their pregnancy, they will find a way, even if it’s unsafe,” she said. “If you can provide access to safe services, women are going to avail themselves of that. Making sure that there is access to safe services will result in saving lives.”
Her view is backed up by studies in countries such as South Africa, where abortion was legalized in 1996. The number of unsafe abortions declined by about 90 per cent in the first two years after legalization, studies found.
In a speech last month, Ms. Gould described her government’s feminist international assistance policy as “the single most important innovation” in Canada’s foreign aid since the late 1960s. “A women’s right to choose and her ability to access family planning and safe abortion services is fundamental to achieving a more equitable, more peaceful and more prosperous world,” she said in the speech.
Not everyone has been equally impressed by the feminist assistance strategy. The McLeod Group, an independent Ottawa-based association of scholars, civil society leaders and former bureaucrats with experience in international development and foreign policy, said the feminist strategy could be perceived as “little more than virtue-signalling” because of a lack of “meaningful new resources” and persistent questions about how to implement the strategy and measure its impact.
Rebecca Tiessen, a professor in the University of Ottawa’s School of International Development and Global Studies, says the feminist assistance policy “offers great potential to fulfill principles of justice and equality for all.”
But while its feminist language is new, its goals are often too vague, she wrote in a policy paper in December. “It does not define feminism, an omission which sets the policy up for built-in vagaries and ambiguity,” she wrote.
On the ground in Mozambique, however, the strategy seems to be making a difference, especially at a time when other donors are cutting back as the Trump policy takes effect.
“Canada stepping in and increasing their funding in this critical area was really a morale booster,” Dr. Mai said.
“A lot of countries are shifting to the right and aren’t paying attention to the development aid needs of women and girls.”
Mozambique has become the biggest recipient of Canada’s funding for sexual and reproductive health and rights, federal officials say. Its needs are substantial. Mozambique has the 10th-highest rate of child marriage in the world, with nearly half of women married by the age of 18, and nearly a third of women say their partner alone makes the family-planning decisions for them, Pathfinder says.
Contraception use has increased substantially in Mozambique, but nearly a quarter of married women still have an unmet need for modern contraception – that is, they want to prevent a pregnancy but cannot obtain modern contraception – according to UN surveys cited by the Guttmacher Institute, a U.S.-based research organization.

On a recent morning in Chimoio, a dozen young women were sitting in plastic chairs under a mango tree with an ativista (activist) from a local organization that participates in the Canadian program. The women, mostly 19 and 20 years old, meet here every two weeks to discuss contraception, family planning, gender violence, child marriage and abortion.
Zaida Gildo, 19, tells the group about a former boyfriend who was unwilling to let her use contraception or continue her education. “There was no future with him, so I washed my hands of him and let him go,” she tells the other women as they laugh in sympathy.
Until recently, most of the young women in the group were unaware that abortion had been legalized. Media coverage of the new law has been minimal, and the government has done little to publicize it. Many of the women can remember friends or classmates who suffered injuries or even death from unsafe abortions, often by taking gruesome home remedies that led to hemorrhaging.
In their meetings with project activists, they learned for the first time that abortion was legal. “Now we realize it can save lives, and it’s not punishable,” Ms. Gildo said. “You have to go to a health facility, with a relative if you’re a minor.”
But when people learn about it, the new abortion services have been popular. At the Manica district hospital, Dr. Diomba did not know about the new law until she received training from the Canadian-funded project in January, 2019. Now the hospital does three or four abortions each day, on average.
During debates in Canada when the former Conservative government introduced its multibillion-dollar maternal-health plan, the prime minister at the time, Stephen Harper, said abortion was too “divisive” in the recipient countries to include in the plan.
Yet there has been almost no backlash to the abortion services in Mozambique, according to doctors and nurses who provide them. No protests or complaints have emerged at their health facilities so far, Dr. Diomba and Ms. Paulo said.
Surprisingly, even Muslim and Christian leaders have accepted the Mozambique project. Activists were able to win their support, partly by finding passages in the Koran and the Bible that could be interpreted as endorsing family planning and women’s rights.
“We had always thought that religious leaders would be the barrier, but we found that they realized they had to adjust to the times,” Katia Amado, a Pathfinder project director, told The Globe. “It was amazing to hear a Muslim sheik telling us that he’s in favour of safe abortion because it saves lives, and because he wants his daughter to become someone, by staying in school.”

In the rural village of Chinhambudzi, an evangelical Christian named Pita Roque works for Pathfinder on the Canadian-funded project, wearing a shirt with “Canada” on his sleeve. The villagers, he said, traditionally believed that a man’s wealth is determined by the number of children he has. They saw abortion as a crime – which forced village women into secret efforts to find backroom methods, sometimes leading to their death.
But these days, Mr. Roque is using his church’s teachings to persuade the villagers to accept family planning and abortion. “If you have a baby and you can’t take care of it, that’s a sin,” he tells the villagers. “On your farm, you don’t just throw the seeds into the ground. You have to prepare the soil first, and you have to plant carefully.”
At an outdoor gathering in the village of Messica, a 19-year-old woman named Helena Muphondajira carries her two-year-old baby on her back as she listens to a Pathfinder mentor. She asks if she can still do family planning after her first child.
“It’s like a maize field – you have to space the plants, so that they have room to grow,” the mentor, Sylvia Desiderio, tells her.
While most sessions are for women and girls only, Pathfinder also organizes discussions with young men. Almost 11,000 men have participated so far.
Sitting around the front steps of a home in Chimoio, two activists lead a dozen young men in a discussion of child marriage. They display a large banner, showing two parents giving their adolescent daughter to an elderly man in exchange for a bride price, and the men discuss the scene. “She’ll be like a slave, and she won’t even be allowed to talk at home,” says Abiola Abraham Zuaga, a 22-year-old student.
The activists tell the men about a new national law, banning anyone under the age of 18 from marrying. They talk about how to report such cases to the police. After an hour, an activist leads the young men in a chant: “For health, for rights, for equality, for the future!” Then the activists give each of the men a small reward: a batch of condoms. And the session ends – to be continued two weeks later.

The above article was published in The Globe and Mail on February 25th 2020.
Pathfinder relies exclusively on funding from individuals and non-U.S. government entities in order to provide any comprehensive safe abortion care and post-abortion care services.
In short, we cannot continue this life-saving work without your support.
Please, ensure women in need can access lifesaving abortion care. Give immediately >>











